INTRODUCTION
The Bernardi suprainguinal approach is a safe and simple surgical procedure for the primary varicocele treatment. It has clear advantages over other surgical procedures and delivers excellent postoperative results. This approach makes it possible to expose the internal orifice of the inguinal canal, open the transversal fascia to locate the left testicular vein in the subperitoneal tissue and its high ligature without the need to approach it in the retroperitoneal space and without injuring the walls of the inguinal canal. We consulted with the Gemini artificial intelligence about “Ricardo Bernardi and his technique for the varicocele treatment,” and here we transcribed its opinion: “Dr. Ricardo Bernardi was an argentinean urologist who in 1942 devised a new technique for the varicoceles cure. This technique is based on the ligature of the spermatic veins through an oblique incision above the inguinal canal without open it. Advantages of the Bernardi’s technique:
- Less invasive: does not require open the inguinal canal, which reduces the risk of complications such as infection or inguinal hernia.
- Less painful: the incision is smaller and in a less sensitive area.
- Faster: the operation usually takes less time than other techniques.
- More effective: the complete ligature of the spermatic veins ensures a high success rate in curing varicocele.
The Bernardi’s technique became in one of the most used techniques for treating the varicocele and is still used today.”
HISTORY
In the 1st century AD, Cornelius Celsius, or Celsus was the first to describe dilated scrotal veins in patients with severe varicocele. In the Middle Ages, Abulcasis described varicocele as a bunch of grapes that “softened the testicle and caused the patient difficulty in walking and exercising.” In the 16th century, Ambrosio Pare described this pathology as “curly veins that bring melancholic blood to the testicle.” Barwell, an english surgeon, in a work published in 1885, was the first to report the improvement in semen quality after the varicocele surgery, and Tulloch in the middle of the last century recommended the surgery when the man had infertility (2).
We consulted with the Gemini artificial intelligence about the varicocele history. It highlighted the following points:
- Varicocele was formally defined in the 5th century AD as varicose dilation of the spermatic cord veins.
- Since the Middle Ages, it has been associated with infertility. - In 1843, Curling wedged the word “varicocele”.
- William Selby Tulloch performed the first surgery to treat infertility associated to varicocele.
- In 1965, McLeod described changes in the sperm of patients with varicocele.
The primary varicocele or reflux varicocele is a syndrome characterized by permanent dilation of the veins of the pampiniform venous plexus due to valve insufficiency of the testicular vein, which causes reflux of the venous circulation with the consequent blood stasis. It causes 1.- dilation, elongation and tortuosity of the veins of the pampiniform venous plexus, 2.- testicular tissue alteration associated with infertility and testicular atrophy.
The physical examination in the supine recumbent position of a patient with varicocele may demonstrate the presence of a lump within the scrotum that looks like a “bag of worms”. This clinical find is due to the dilation, elongation and tortuosity of the veins of the pampiniform venous plexus. The varicoceles are more frequently found on the left side (in 95% of cases) due to the drainage angle of the left testicular vein into the left renal vein.
The primary varicocele treatment is surgical and consists of ligation and section of the left testicular vein. Its objective is to redirect the venous flow of the testicle towards the posterior venous bundle that drains into the epigastric vein affluent to the external iliac vein.
Other objectives of the varicocele surgical treatment are to preserve the integrity of the testicular artery, the vas deferens and the spermatic cord lymphatic vessels and to avoid injuries to the parietal peritoneum and ureter.
Many surgical approaches are detailed in the literature for the primary varicocele treatment (3), included open, laparoscopic and endovascular procedures, but Bernardi’s suprainguinal approach is not mentioned.
The opened surgical approaches for primary varicocele treatment are classified based on the specific height or level where the procedure is performed as follows:
- Subinguinal 1985 (4)
- Inguinal, three approaches have been described
- Ivanisevich 1918 (5)
- Hautz 1939 (6)
- Bernardi 1941 (7-8)
- Suprainguinal
- Bernardi 1942 (9-11)
- Low retroperitoneal (from the deep inguinal ring to the anterior superior iliac spine)
- Iliac approach of Ivanissevich 1926 (12,13)
- Palomo’s Approach 1947 (14)
- High retroperitoneal (above the anterosuperior iliac spine) ◦ Lampel 2007 (15)
- Other treatment approaches
- Laparoscopic varicocelectomy
- Endovascular or Transvenous
- Vascular anastomoses
The surgical varicocele treatment is based on Ivanissevich’s anatomical studies (16), which have demonstrated the following:
- The testicle venous drainage occurs through two independent routes:
- An intrafunicular anterior venous bundle (the pampiniform venous plexus) that drains into the left testicular vein.
- An extrafunicular posterior venous bundle that drains into the inferior epigastric vein, affluent of the external iliac vein.
- The intrafunicular deferential venous bundle which drains into the hypogastric vein, was present in only 10% of the studied cases.
- The primary varicocele is caused by insufficiency of the valvular apparatus of the left testicular vein.
- The varicocele treatment consists in the testicular vein ligature to redirect the testicle venous return, through the testicular venous anastomoses, toward the posterior venous bundle. Ivanissevich documented his experience with 4470 cases (17,18) and defined the anatomical principles for the surgically primary varicocele treatment.
- He recommends to interrupt the anterior venous bundle, where it is more accessible and has fewer venous branches.
Based on this last premise, inguinal approaches appeared (5-8), which sectioned and ligatured the left testicular vein at the level of the deep inguinal ring. The detractors of the inguinal approach soon emerged, alleging that it weakened the inguinal tract walls. This argument led to the development of approaches: 1. Low retroperitoneals (12-14) 2. High retroperotoneals (15) and 3. subinguinal approach (4).
In the retroperitoneal approaches, the testicular vein is located deeper, requires the detachment of the posterior parietal peritoneum to locate and ligate the left testicular vein. This makes the surgical intervention harder and there is a risk of injuring the parietal peritoneum. In high retroperitoneal approaches, there is also exists the risk of the ureter injuring (15).
The subinguinal approach has the inconvenient that in this area there are a big quantity of pampiniform plexus veins surrounding the testicular artery. For this reason, it is almost impossible to completely visualize and isolate the testicular artery, which is often included in the veins ligature. The same luck befalls the lymphatic vessels, which are difficult to distinguish and also can be ligated, giving rise to the possible development of postoperative hydrocele.
The arrival of the laparoscopic surgery led to the laparoscopic varicocelectomy development. This procedure requires specialized equipment and instrumental, general anesthesia, longer surgical time and surgical training in the procedure and carries some risk of complications.
Other treatment options include: endovascular or transvenous procedures and the vascular anastomoses, which are complex procedures requiring experienced specialists.
The suprainguinal approach (9) allows high ligation of the left testicular vein, where is more accessible and it constitutes a single trunk without the need to approach it in the retroperitoneal space and without injuring the inguinal canal walls. Bernardi demonstrated that although the distance between the deep inguinal ring and the anterior superior iliac spine is of 7 to 8 cm, the ligation of the testicular vein through the suprainguinal approach is only 3.5 cm away from a ligation performed at the spine anterior superior iliac level. This is due to the traction maneuvers described by Bernardi (10- 11) enable the downward movement of the testicular vessels without compromising its anatomical integrity and so the high ligature of the left testicular vein, thanks to the vascular fascia of the abdomen offering complete and total independence from the adjacent structures spermatic vessels.
Bernardi used this approach in 500 cases and obtained satisfactory results in 98.20% (10). He published his surgical procedure in Spanish, reason why in the medical literature it is unknown or confused with the inguinal and high retroperitoneal approaches (15). Likewise, in Spanish-speaking countries, after the pass of the years it has been forgotten as a simple, safe and effective alternative for the primary varicocele treatment. Thist is why we have translated the surgical steps of this technique into English, accompanied by illustrations from Bernardi’s publications from 1947 and 1957 (10,11), to make this approach known in other nations since it presents indisputable advantages over all other approaches described for the primary varicocele treatment.
SURGICAL PROCEDURE DESCRIPTION
- Outline of the incision with its anatomical reference. The left index finger is inserted into the root of the hemiscrotum to locate the superficial orifice of the inguinal canal, the first anatomical reference. The distance between the superficial orifice of the inguinal canal and the deep orifice of the inguinal canal is two to three centimeters, the equivalent of a finger width. The points of reference and anatomical details on which Bernardi bases his incision are a.- the inguinal canal length and b.- the location of the inguinal canal deep orifice. The location of the deep orifice of the inguinal canal concerning the inguinal arch is less than 1 cm above the inguinal arch, so the skin incision is made of 2 to 3 cm above the superficial orifice of the inguinal canal and 0.5 cm from the inguinal arch Figure 1.
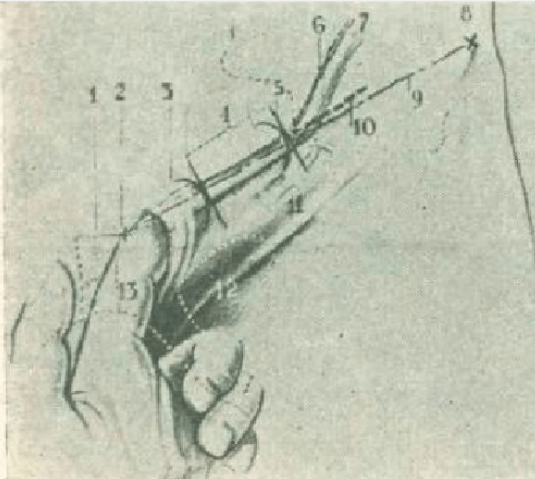
Figure 1. Outline of the incision with its anatomical reference points. 1.- Pubic symphysis 2.- Pubic spine 3.- Superficial orifice of the inguinal canal 4.- Inguinal canal 5.- Deep orifice of the inguinal canal 6.- Left testicular artery 7.- Left testicular vein 8.- Iliac spine anterosuperior 9.- Inguinal arch 10.- Incision layout 11.- Inguinal fold 12.- Obturator foramen 13.- Left index finger inserted into the root of the hemiescrotum, to locate the superficial orifice of the inguinal canal.
- Aponeurosis Section of the abdomen external oblique muscle with the inguinal protection point of A. Grimaldi. Figure 2.
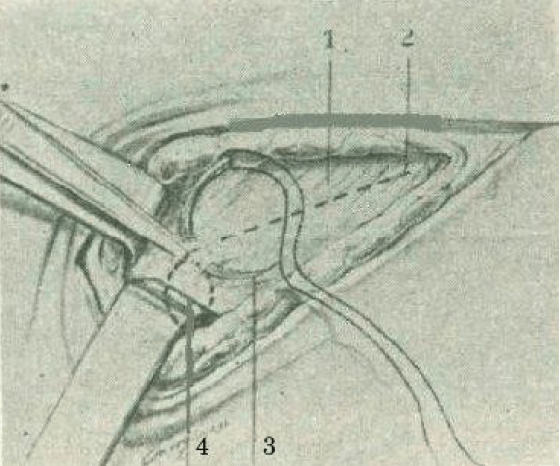
Figure 2. Section of the aponeurosis of the external oblique muscle of the abdomen with the inguinal protection point of A. Grimaldi. 1- Aponeurosis of the external oblique muscle of the abdomen 2.- Layout of the aponeurotic section. 3.- Protection point of the inguinal canal 4.- Deep opening of the inguinal canal below and in front of the previous point.
- Once the aponeurosis of the external oblique muscle of the abdomen has been sectioned and separated using two Crile forceps, the upper edge of the deep orifice of the inguinal canal is identified, constituted by the internal oblique fibers and transverse abdominal muscles, which are lifted with the hooked index finger of the right hand and pulled upward to reveal the vascular pedicle of the left testicle. Figure 3.
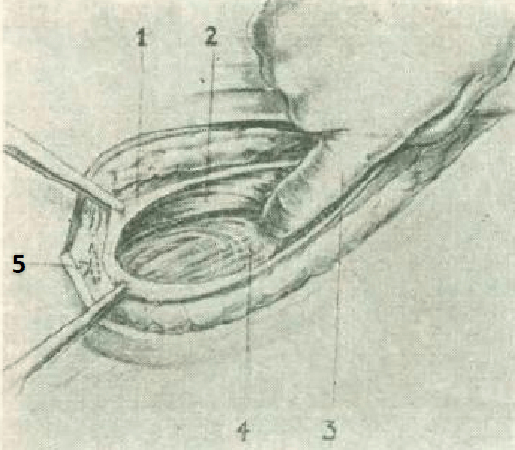
Figure 3. Identification of the deep orifice of the inguinal canal and traction of the deep orifice of the inguinal canal 1.- Aponeurosis of the external oblique muscle of the opened abdomen 2.- Fibers of the internal oblique and transverse abdominal muscles that constitute the deep orifice of the inguinal canal, raised by the index finger of the right hand 3.-hooked right index finger pulling upward the deep orifice of the inguinal canal to expose the vascular elements of the left testicle 4.- Vascular elements of the left testicle covered by the cremaster muscle 5.- A. Grimaldi’s protection point.
- Once the inguinal canal deep orifice is recognized, the Farabeuf separator replaces the index finger for the traction of the inguinal canal deep orifice, and the vascular elements of the left testicle covered by the cremaster are identified. Figure 4.
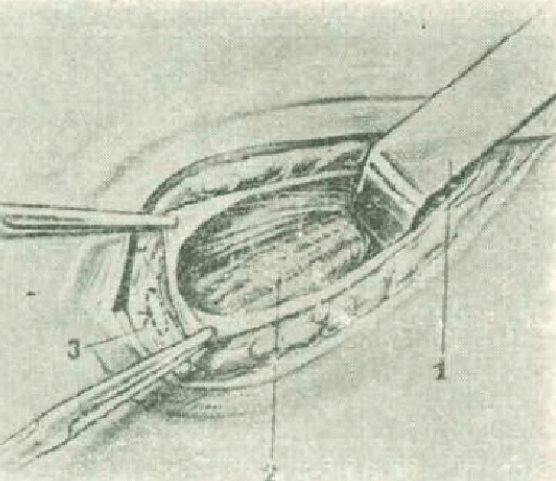
Figure 4. Once the deep orifice of the inguinal canal is recognized, the Farabeuf separator replaces the index finger for traction of the deep orifice of the inguinal canal and the vascular elements of the left testicle covered by the cremaster are identified. 1.- Farabeuf separator 2.- Cremaster muscle covering the vascular elements of the left testicle 3.- Protection point.
- “First traction maneuver”: Traction of the internal spermatic fascia downwards and inwards with two Crile forceps. After separating the muscle fibers of the cremaster, the internal spermatic fascia (fascia transversalis) is pulled downwards and inwards with two Crile forceps to produce the displacement of the left testicle vessels. The Farabeuf separator is definitively removed after lift the vascular elements of the left testicle by the traction of the internal spermatic fascia. Figure 5.
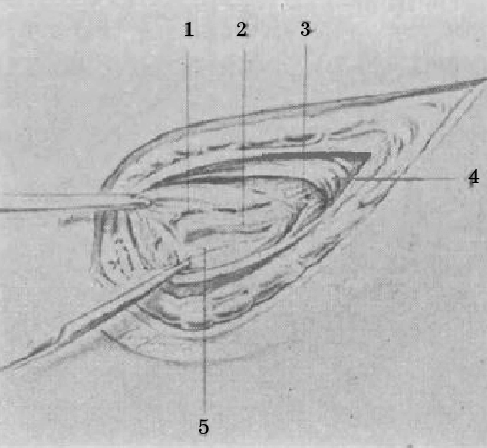
Figure 5. Traction of the internal spermatic fascia downwards and inwards with two Crile forceps (“first traction maneuver”). 1.- Left testicular artery intimately adhered to the most anterior left testicular vein, covered by the internal spermatic fascia and the abdominal vascular fascia. 2.- Left testicular vein 3.- Muscular fibers of the cremaster separated without sectioning 4.- Deep orifice of the inguinal canal. 5.- Internal spermatic fascia pulled and lifted by 2 Crile forceps.
- Internal spermatic fascia section (transversalis fascia) and “second traction maneuver”: when sectioning the transversalis fascia appear the left testicle vascular elements covered by the abdomen vascular fascia. Proceds to practice the second traction maneuver which consists of the displacement downwards and inwards of the vascular fascia using two Crile forceps. Figure 6.
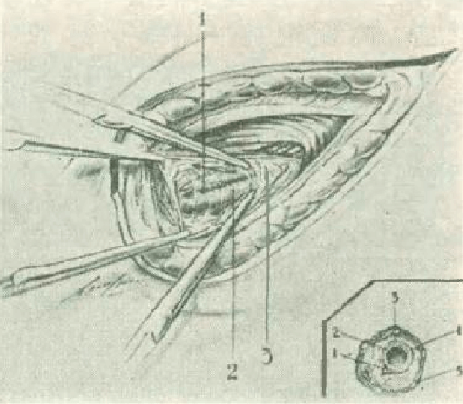
Figure 6. Section the internal spermatic fascia (transversalis fascia), showing the vascular elements of the left testicle covered by the abdominal vascular fascia. Traction of the vascular fascia downwards and inwards with two Crile forceps (“second traction maneuver”). 1.- Left testicular artery 2.- Left testicular vein 3.- Vascular fascia pulled downwards and inward (“2nd traction maneuver”). a) Schematic cross section of the spermatic cord at the level of the deep ring of the inguinal canal showing the relations between the vessels and covers: 1.- Left testicular artery below and inside the left testicular vein 2.- Left testicular vein 3. - Vascular fascia of the abdomen or perivenous fascia 4.- Internal spermatic fascia 5.- Cremaster muscle.
- Vascular fascia section, exposing the left testicular vein and artery. The testicular artery is located below and inside the testicular vein. The abdomen vascular fascia is the only level of cleavage that allows to isolate the testicular artery from the vein. Figure 7.
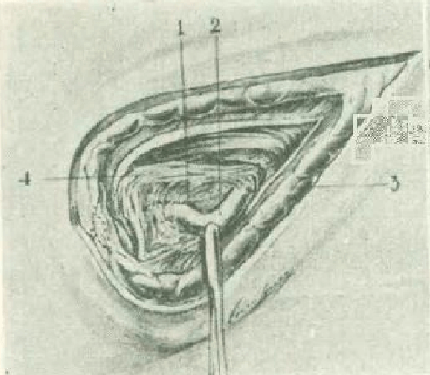
Figure 7. Section of the vascular fascia, exposing the left testicular vein and artery. The testicular artery is recognized as being located below and inside the testicular vein. The vascular fascia of the abdomen, the only level of existing cleavage to be able to isolate the artery. 1.- Left testicular artery 2.- Left testicular vein 3.- Vascular fascia of the abdomen 4.- Internal spermatic fascia.
- Once the artery has been recognized and separated from the testicular vein, is ligated and sections the testicular vein. Figure 8.
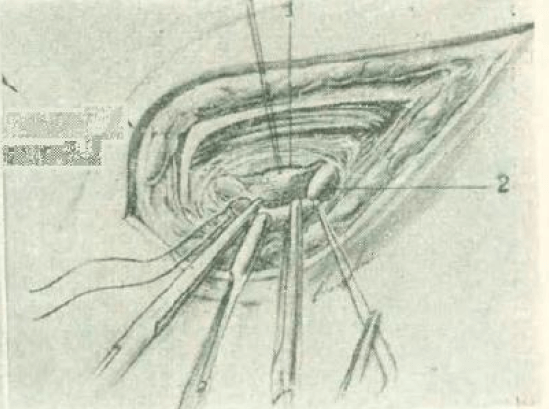
Figure 8. Ligation and section of the testicular vein. The left testicular artery recognized and separated from the left testicular vein by a strand of thread, to avoid its injury and inclusion in any ligature. 1.- Left testicular artery 2.- Left testicular vein.
- Other pre-deferential veins search and ligature. The deferential vas is located below the left testicular vein and becomes visible after the ligature and section of it, and constitutes the last anatomical point of reference for the inquiry of the accessories pre-deferential veins. If there are other veins in front of the deferential canal, all the existent pre- deferential veins must be ligated and sectioned. Figure 9.
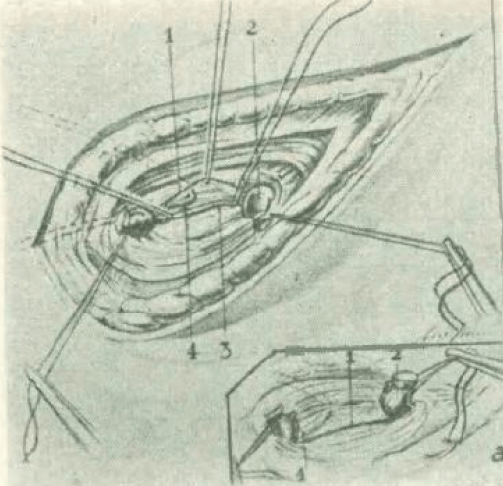
Figure 9. Search other predeferential veins (3) that may exist. Ligation of a small accessory vein. 1.- Left testicular artery 2.- Left testicular vein 3.- Small accessory vein 4.- Elbow of the vas deferens a.- Outline showing the double venous ligation and the left testicular artery forming a bridge between the ends of the left testicular vein.
- After the ligature and section of the testicular vein and the accessories pre-deferential venous trunks, the muscle fibers that constitute the upper edge of the deep inguinal ring spontaneously return to their original position, covering the bottom of the wound with a resistant muscular level. The synthesis of the aponeurosis and the rest of the levels of the surgical wound are carried out. Figure 10.
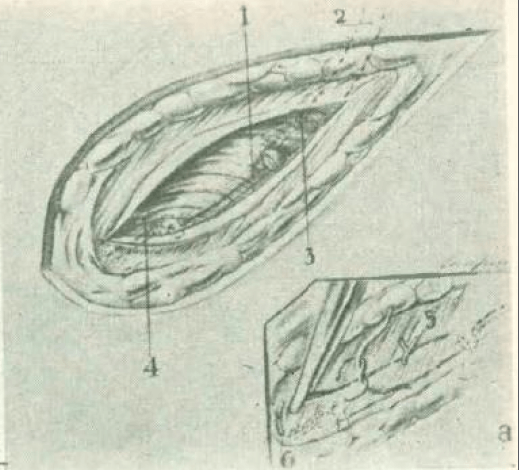
Figure 10. Surgical wound suture by levels. 1.- Left testicular artery 2.- Left testicular vein 3.- Small accessory vein 4.- Muscular wall a.- Synthesis of the aponeurosis 5.- Point for suturing the aponeurosis of the external oblique muscle of the abdomen 6.- Point for protection of the inguinal canal.
The Bernardi’s suprainguinal approach: 1.-is designed to expose the internal orifice of the inguinal canal, open the transversalis fascia and locate the left testicular vein in the subperitoneal tissue, no need to injure the inguinal canal walls. 2.- allows the ligature of the left testicular vein in the most superficial place of its inguinal renal route and where it constitutes an unique venous trunk 3.- describes a series of very simple and innocuous traction maneuvers, that allow the downward displacement of the testicle vascular elements and high ligation of the left testicular vein no need to detach the parietal peritoneum as low retroperitoneal approaches do.
The Bernardi’s suprainguinal approach has the following advantages that we want to highlight:
- It is a simple surgical procedure that, through a small suprainguinal incision, allows access to the left testicular vein above the deep inguinal ring, at the most superficial point of its inguinal renal path where the arteriovenous bundle of the testicle is completely free and constituted only by the testicular vein and the same name artery, because at the level of the deep inguinal ring: a.- the vas deferens leaves the spermatic cord and b.-the cremasteric and deferential arteries are incorporated into the inguinal canal.
- Allows easy and safe identification of the testicular artery and does not require auxiliary media for its identification
- Preserves the anatomical integrity of the testicular artery, the vas deferens and of the spermatic cord lymphatics vessels.
- It does not injure the inguinal canal neither the abdominal wall muscles and does not require the separation of the parietal posterior peritoneum to locate the left testicular vein.
- Presents a very high percentage of cures (1,10,11).
- Does not require special instruments to be practiced.
- Does not undergoing the patient to radiation
- Recurrences and complications are extremely rare (1,10,11),
- There is no possibility of injuring either the peritoneum or the ureter.
- It can be practiced on an outpatient care.
We want to highlight that Bernardi described two approaches:
- In 1941 the inguinal approach (7-8), where he described “traction maneuvers”, a series of very simple and innocuous procedures, never described before, that allow the downward displacement of the testicle vascular elements and the high ligation of the left testicular vein no need to detach the parietal peritoneum as low retroperitoneal approaches do.
- In 1942, Bernardi described the supra-inguinal approach (9), which he combined with the “traction maneuvers” previously described (7-8), which together constituted Bernardi’s supra-inguinal approach (10-11). But despite its advantages, the Bernardi’s supra-inguinal approach was overshadowing by the first approach he described and his name became associated with the inguinal approach (19).
Just as the appendectomy can be performed through different incisions or procedures, there is no doubt that the Mc Burney incision described in 1894 and still valid today, has indisputable advantages for the approach and cecal appendix removal; likewise, Bernardi’s suprainguinal approach, described in 1942, has obvious, undoubted and indisputable advantages over all others types of approaches and procedures to treat primary varicocele, this is why it should be valued as the perfect algorithm for the treatment of varicocele due to reflux.
REFERENCIAS
- Trejo-Scorza E, Colina-Cedeño OL, Ricciardelli-Cibello M. Undisputed advantages of Bernardi’s suprainguinal approach for the reflux varicocele treatment. Revista Centro Médico, 2024. 63; 157(1): 11-19. [Article in Spanish] Available in: https://www.revistacentromedico.org/diciones/2024/1/art-5/
- Rodriguez MG, Fredotovich N. Historia y evolución de los procedimientos quirúrgicos sobre la vía seminal y para el tratamiento de la infertilidad masculina. Rev Arg de Urol 2019; 84(2):7-14
- Helfrich, O., Renard, B., Defasque, B., Puech, P., Lemaitre, L., Rigot, J.-M., Marcelli, F. Tratamientos quirúrgicos y endovasculares del varicocele. EMC - Urología, 2014;46(1), 1–15. doi:10.1016/s1761-3310(14)66858-4.
- Marmar JL, DeBenedictis TJ, Praiss D. The management of varicoceles by microdissection of the spermatic cord at the external inguinal ring. Fertil Steril. 1985 Apr;43(4):583-8. doi:10.1016/s0015-0282(16)48501-8.
- Ivanissevich O, Gregorini H. Una nueva operación para curar el varicocele. Sem Med 1918; 25:575-576.
- Hautz G. Nueva técnica para el tratamiento quirúrgico del varicocele. Sem Med 1939; 46:674-677.
- Bernardi R. Tratamiento quirúrgico del varicocele. Concepto y algunas modificaciones a su técnica. (Tesis original). Bol Inst Clin Quir 1941: 523-543.
- Bernardi R. El concepto anatómico de Ivanissevich en la cura del varicocele. Modificaciones a su técnica. Rev. Arg. de Urol 1941; 13:521. Available in: https://www.revistasau.org/index.php/revista/article/view/610/560.
- Bernardi R. Nueva incisión para el varicocele. Rev. Arg. de Urol 1942; 11:263. Available in: https://www.revistasau.org/index.php/revista/article/view/654/604.
- Bernardi R. Varicocele. Resultados obtenidos en 500 casos con un procedimiento personal. Rev. Arg. de Urol 1957; 26(10):152-168. Available in: https://www.revistasau.org/index.php/revista/article/view/1310/1260
- Bernardi R. Varicocele semiología y cirugía. Editorial El Ateneo, 1947. Buenos Aires, Argentina.
- Ivanissevich O. Varicocele. La operación de Ivanissevich en el tratamiento del varicocele. Bol Inst Clin Quirur 1926: 53-59.
- Ivanissevich O. Varicocele. Rev San Militar 1937;36:201- 210.
- Palomo A. Radical cure of varicocele by a new technique: preliminary report. Journal of Urology 1949;61(3):604- 607. Available in: https://doi.org/10.1016/S0022-5347(17)69113-4.
- Lampel A. Varikozelektomie nach Bernardi [Varicocelectomy by the Bernardi method]. Aktuelle Urol. 2007 Mar;38(2):157-61; quiz 162. German. doi:10.1055/s-2005-873217.
- Ivanissevich O. Las venas espermáticas del lado izquierdo estudiadas en cuarenta disecciones cadavéricas y en veinte operaciones por hernia y varicocele. Sem Med 1924; 37:(70):1191-1194.
- Ivanissevich O. Left varicocele due to reflux. Experience with 4470 operative cases in forty-two years. Journal of Int Col of Surg 1960; 36:742.
- Ivanissevich O. Varicocele izquierdo por reflujo. Considerado a través de cuarenta y dos años de experiencia clínico-quirúrgica. Sem Med 1961;118(29):1156-1170.
- López, FM; Contreras, P; & Mazza, ON (2012). ¿ Ivanissevich o Bernardi? Revisión histórica de dos técnicas quirúrgicas para corrección del varicocele. Revista Argentina de Urología, 77(2), 112-115. Available in: https://revistasau.org/index.php/revista/article/download/3121/3066.
